Consensus community valuation
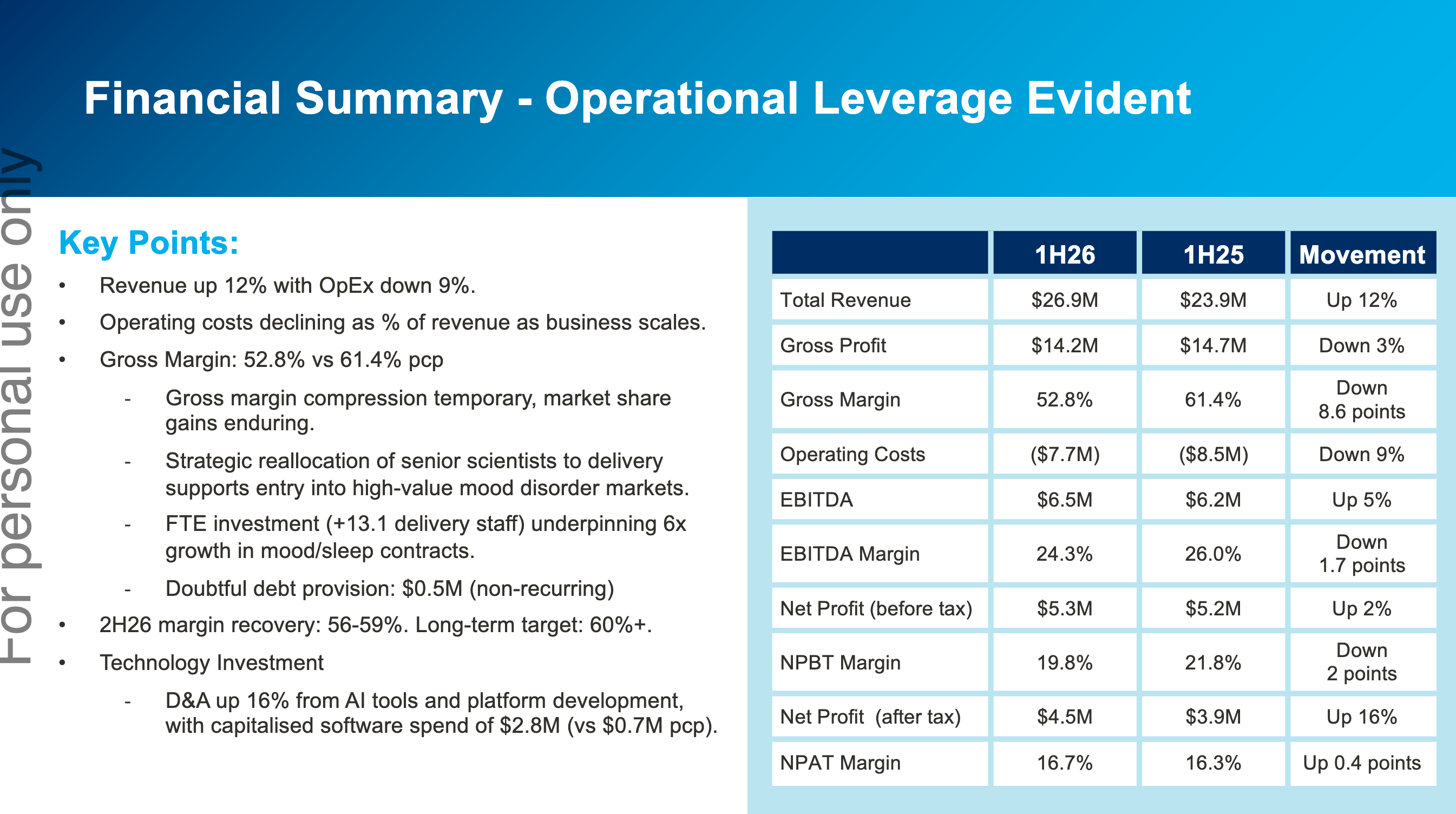
It was a solid, though unspectacular half. There’s been a bit of margin pressure due to increased investments which have been flagged 6 months earlier. They’ve flagged for a stronger second half based on significantly higher contracted revenue on hand verses this time last year.
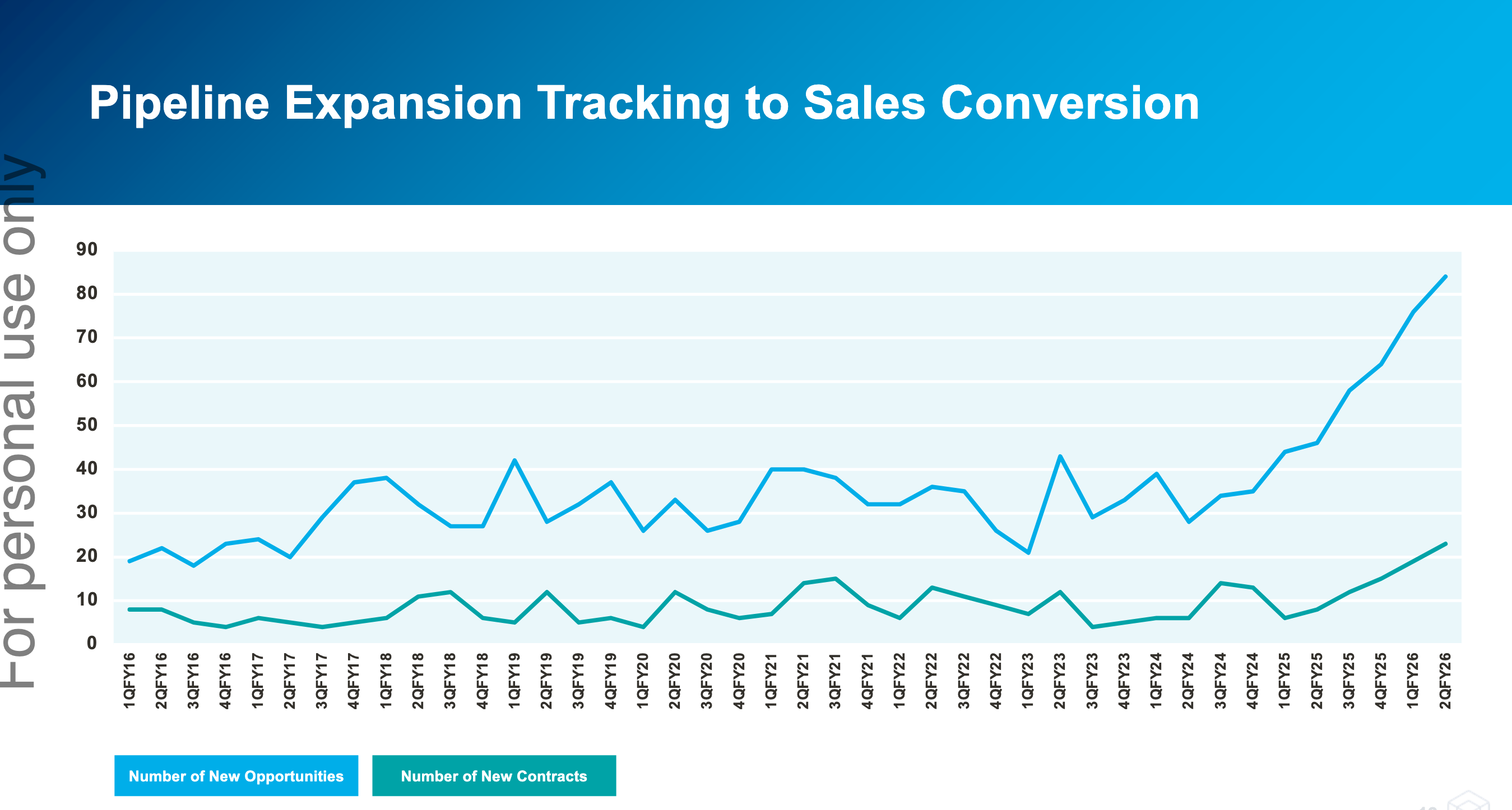
While the current results are subdued, the outlook has never been brighter. The number of new opportunities and new contracts is breaking out. Management has previously stated that contract wins lag opportunities by ~9 months, but there’s evidence that contract wins are now also starting to tick up.
A lot of this is due to expansion into new indications outside of Alzheimer’s Disease (AD) and work from the partner channels, specifically Medidata. Partner channels were 62% of new contracts in Q2 - I estimate it was less than 30% in Q1 and even lower previously. These new contracts are smaller in size, but are faster to execute, are more predictable and less prone to unexpected delays.
Reading through some of the old straws, it’s evident that a lot of investors were put off by how dependent the company was in winning large Phase 3 AD contracts. These contracts are large, concentrated, incredibly lumpy and prone to unexpected delays.
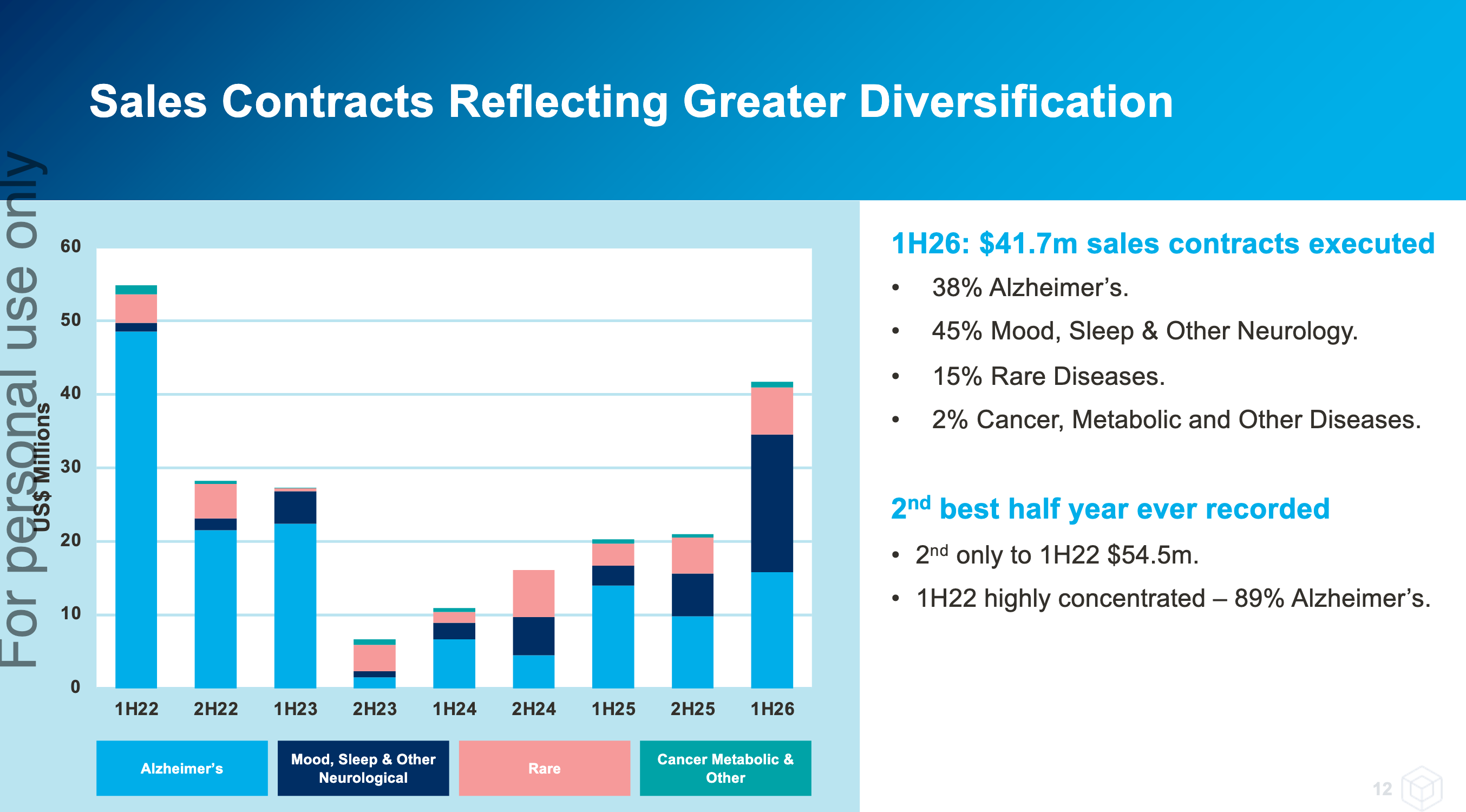
However Cogstate’s last large Phase 3 AD win was in FY22, and they’ve proven they can grow without these. And as new contract wins have shown, non-AD contracts are forming the “cake” of the growth story while AD contracts have been relegated to the cream and cherry on top.
By the way, the opportunities for large Phase 3 AD wins have not disappeared. The CEO has been hinted that he expects to see new Phase 3 pre-clinical AD contracts (which CGS has a very high win rate) to be rewarded in CY 2026. My bet is Roche’s upcoming PrevenTRON trial, or a brand new trial from Eli Lilly.

Looks like they "beat" the downgraded forecast for 1H FY26 that was given just a month ago

A couple of things to note.
1) They're diversifying into other non-AD indications. These are also small and faster to execute trials, which make the business more predictable. From conversations with management, they're still hinting at a large AD win not too far in the horizon - so there's no visible deterioration in competitiveness there, it's just big and lumpy.

2) They've always recognised license revenue upfront. But now they're starting to do it across the length of the trials. I believe this is only for the new endpoints they've developed. Will smooth out revenues are bit more, and probably made 1H FY26 look a little worse, particularly on the margin side of things (license is 90%+ GM vs ~50% GM for services).

It was a great set of results for FY25. Though much of it was pre-announced in an earlier trading update, so there were no surprises. 2H was significantly stronger with $27.9m revenue and $8.1m EBIT. A notable shift from prior years is the growing share of smaller clinical trial wins, which provide faster turnarounds and earlier revenue recognition.

In the past, Cogstate has hinted that channel partnerships (with groups like ERT or Clario) could help drive sales. It now looks like they’ve found the real deal in Medidata - a major electronic data capture company with 4,000+ staff and roughly 800 salespeople. The partnership is still in its infancy: the sales team only began ramping up in February 2025, yet proposals involving Medidata already represent around 20% of Cogstate’s pipeline. With Medidata’s far deeper reach into clinical trials, Cogstate is accessing a broader range of opportunities than it could on its own. Management has made it clear this is only the beginning, with expectations of further pipeline growth and contract wins as the joint approach matures.
We’re also beginning to see the benefits of the April 2024 licensing amendment with Japanese pharma giant Eisai, which returned global rights to Cogstate’s assessment technology. That technology is now being used to help pharma companies pre-screen patients for clinical trials - an application that generated $1.2m in FY25 revenue, with more opportunities of this kind already in the pipeline.
It’s been a tough stock to hold over the years, largely because Cogstate has been so reliant on a small number of large phase 3 Alzheimer’s trials. The scarcity of these large deals, combined with their inherent lumpiness and the impact of patient recruitment delays, has led to significant year-to-year swings in the company’s performance.
All of a sudden, the outlook looks much brighter. The business is diversifying beyond Alzheimer’s into areas like rare disease, sleep disorders, and Parkinson’s - smaller trials that are quicker to secure and faster to recognise revenue from, smoothing out the historic lumpiness. Medidata is now driving meaningful RFP flow and opening doors into new indications. Cogstate has also began monetising its consumer-facing technologies for patient recruitment, with scope to expand into further use cases. Importantly, the upside from large phase 3 Alzheimer’s trials remains intact, with a number of big pharma companies currently progressing phase 2 programs.
Management have suggested revenue growth is once again expected in FY26, but with the shortened sales cycles and revenue recognition, no specific numbers have been given. Also expect a modest margin decline (~0-3 percentage points on EBITDA/EBIT) due to increase investments. They’re off to a strong start with $14.1m of contract revenue banked since June 30. A maiden $0.02/share fully franked dividend was also declared.
One could make the case that it’s a very reasonably priced company with an EV/E of 15x (annualise 2H performance), that’s more self-reliant than it has previously been (broader beyond AD, stronger channel-partner leverage, and a faster cadence of smaller contracts), with some tremendous tailwinds (pursuit of AD treatments, pharma chasing earlier stages of AD that require more sensitive endpoints, etc). Ultimately, this is only for investors that have belief in the long-term tailwinds and willing to ride the bumps and grinds - this is not your grandad’s SaaS company adding incremental ARR every year.
For those that may have missed this last week - Cogstate (CGS) came out with a fairly decent guidance upgrade last week.

So if we take the mid-point of $13m PBT should give us earnings of about $9.1m (30% tax rate).
There is circa 169 million shares in issues which then provides about $0.054 EPS.
At current SP = ~$1.71 / 0.054 = a PE of roughly 32.
With CGS returning to growth this seems fairly on point, but you'd expect/want to see this continue into FY26.
Will be an interesting annual report to review.
Feel free to jump in and add to the above.
Didn't know that Cogstate was part of the ASX300 as I thought the rule was trading the top 300 shares.
Or they've made a new rule none of us knows about.
Anyway it is there if anyone wants to try their luck.

UPDATE - Feb 2023
*all figures in US dollars unless otherwise stated*
Readjusting some of my forecasts in preparation for Cogstate's upcoming H1 report. My 2023 forecasts were well off, primarily due to delays with closing out contracts. I forecasted 10m FCF; instead they were in the negatives (gulp). That said, management have suggested these issues are no longer current, and with some additional cost savings expected, I am hoping to see improvements to cash flow.
I am dropping my FCF forecast (for FY24) to 8.5m. I am also increasing my discount rate to 10%. Cogstate's buyback has seen shares decrease to around 171m -- call it 172m to be conservative. As for future cash flow forecasts, I have dialled these back somewhat to provide more safety in my valuation: 11.5m in FY25, 13.5m in FY26 and 15.5m in 2027.
Noting the above, I reach a company value of 246m. Divide this by shares outstanding and I reach a valuation of US$1.10, or 1.70 converted to AUD. Provided Cogstate continues to grow strongly, I think shares are attractively priced. If you remove growth to cash flows though, all of a sudden a share price of 50c would appear expensive. We NEED to see growth going forward and another year of contract delays or similar won't cut it. I am not suggesting this is likely, but the bear case is always something to keep in mind.
UPDATE - September 2022
*all figures in US dollars unless otherwise stated*
As @Noddy74 indicated a few weeks ago, Cogstate's share price was battered after the release of their FY22 results. As @Noddy74 outlined, FY23's outlook was likely a key reason for this, with management advising of delays to a number of clinical trials. FCF also decreased to 8m (was 14m in FY21), so this was likely a contributor too.
Looking back at my previous valuation, I conservatively estimated that FY22 FCF would be 4.5m -- intentionally providing a huge margin of safety given the lofty valuation at the time.
While FY22 FCF did indeed decrease, it nearly doubled my estimation coming in at 8m for the year. In addition, profit increased from 5m to 7m, cash on hand increased handsomely to 29m, while CapEx costs decreased to -1.6m (previously 1.77m). Clinical trials margins also increased to 60%, up from 54%. Did I mention they have no debt?
I am not buying the business for next year's FCF; I own Cogstate because I think FCF in FY25 and onwards will be much higher than it is today. @Noddy74 touches on revenue backlog in his Straw -- so refer to that for more detail -- but this is not a business with structural concerns; quite the opposite. As the below demonstrates, revenue backlog for FY24 and to a lesser extent FY25 are almost that of FY23. And this is base case -- progress or further development on the Alzheimer front will likely have a serious (positive) impact on future cash receipts.

I forecast FY23 FCF of 10.5m, with this rising to 13.5m in FY24. Similar to my last valuation, I am giving myself plenty of breathing room with what I consider conservative FCF increases. Using a discount rate of 8.4%, I reach a company value of 325m; divide this by shares outstanding (173m) and I reach a current valuation of $1.85.
Cogstate is currently high on my 'top up' list.
_______________________________________________
*all figures in US dollars unless otherwise stated*
FY22 projected revenue: 42m
FY21 revenue: 32.6m
FY20 revenue: 22.7m
Gross margin: 53%
Net profit margin: 16%
Within my DCF I used FCF projections with a discount rate of 8.4%. The company had a cracker of a year last year, achieving 16m in FCF. Q1 and Q2 figures in FY22 suggest CGS’ FCF has dropped (-0.27m and 1.55m respectively). I have forecast 4.5m FCF in FY22, with 2m+ yearly increments recorded thereafter (conservative yes, particularly if the Eisai deal starts to gain traction, but best to be on the safe side noting lumpy results). This gives me a CV of 154m – divide this by shares outstanding and I reach a valuation of 0.90c (or approx. AU1.30c, although the continued drop in the AU dollar doesn't help).
I suspect CGS net profit margins will drop slightly within FY22 results, down to approximately 14%. This is based on the calculation that FY22 profit comes in at around 5.8-6m, which would represent a slight profit increase on FY21 figures.
Let me know if I have missed something in the above calculations.
Now, while my DCF doesn’t exactly provide confidence that current levels are cheap, maybe its true to say that high quality healthcare stocks will always trade at a premium – so to wait for it to reach
That said, there are some negatives too. There has been lots of insider selling in the last 12 months and I am of the belief that the CEO salary is far too high. And with increased costs impacting their FCF in FY22, a bear case can possibly be made.
Disc: held
Not a huge surprise, but good news nevertheless.


Hopefully in the eyes of pharma companies and biotechs this helps de-risk the development of future Alzheimer’s treatments, and in turn increase the demand for Cogstate’s clinical trial products and services. This is the main bull case of the FDA approval for CGS.
Apart from the financial strain to the US government (US$26.5k per year for the treatment), other key concerns involve the strain of the demand to the medical system. PET scans, genetic tests, neurologists, the laborious administration by intravenous infusion every 2 weeks, and so forth.
Cogstate may stand to benefit in a couple of ways. One is the likely follow up clinical trials for Leqembi, and other likely FDA approval candidates, to use less laborious administration of the drug. Perhaps longer intervals or subcutaneous injections instead of infusion.
Two, in order to qualify for Leqembi, prospective patients will need to have cognitive tests completed and submitted to centralised registries. A low-touch digital test would help ease the load on the medical system by opening up the pool of healthcare professionals that can administer them. No doubt Eisai and Cogstate are hoping their upcoming digital apps will play a large role in this.
See my straw in Telix about Lantheus
https://strawman.com/reports/TLX/edgescape?view-straw=22592

Hopefully there isn't much overlap.
[held]
Seems to be good news. Hopefully this will lead to further studies and eventually turbocharge general healthcare use of Cogstate (the latter not being my central thesis).

[Held]


at 25th January 2023:
MC : $346Mill , closed at $2.00 a share

Annual report 2022
AGM 4th Nov 2022


CGS removal:

Noted Sector: Industry Group: Health Care Equipment & Services
Listed on 13 February 2004
............................................................................................................................
at 30/8/22 profitable:
FY22 Financial Results & Business Outlook
EBITDA**: $13,009,201 $5,711,737 $7,297,464 up 127.8%
2022 EPS growth up 40%
Return (inc div) 1yr: 1.50% 3yr: 101.21% pa 5yr: 9.23% pa
Need to check the Outlook for 2022 / 23:
In respect of forecast earnings, Cogstate continues to target EBIT margins in the range of 20% - 24% over the coming years. Based on current revenue forecast, FY23 EBIT margins are expected to be at the bottom end of that range. Target EBITDA range is 27% - 29% of revenue.
A further update will be provided at the company’s AGM on Friday 4 November 2022.
..........................................................................................................

Although Cogstate's quarterly update looked a little underwhelming at first glance, that's mainly the result of cycling a monster quarter (by far the largest in their history) from a year ago. Read a little more into the result and it's actually really strong.
Future contracted revenue is at a record high of US$148.3m after adding a net US$17.9m in the most recent quarter. That is one of the highest net additions in their history. It also meant they went back to filling the top of the sales funnel at a faster rate than it was recognised as income. That is one of the key things I look to with Cogstate to continue to give me confidence they will continue to grow over the longer term.
In terms of short-term performance FY23 is likely to be a slightly muted year. The revenue backlog for FY23 grew from US$33.9m at 30 Jun to US$36.8m as at 30 Sep (including 1Q actuals). They are yet to give guidance but will do so at the AGM. In prior years Cogstate has gotten between 35% and 51% of its revenue from in-year signings. That would point to a full year result of US$52-69m. However, they also stated they expected the contribution from in-year signings to reduce. Overall I think the lower end of that range to be challenging and small beat of the FY22 result of US$45m is probably more realistic. However, FY24 and FY25 continue to look really positive.

They also highlighted the Eisai Lecanemab results that were released last month and have been extensively discussed. Topline results from Roche's Gantenerumab and Lilly's Donanemab are due this quarter and mid 2023 respectively.
Cogstate's AGM is being held on Friday 4 November at 11am, where they will also provide full year guidance.
[Held]
Cogstate reported today with record revenue (up 38% YoY), record profit (up 84%), record clinical sales contracts executed (up 74%) and a record order book (up 37%) at $139.1m. Looking backwards, forwards, up and down it looked pretty good. The share market rewarded them with a trimming of the share price of almost 10% at one point. So what's going on? Let's take a look.
What the market really didn't like was the outlook for FY23. Management highlighted on the call that a number of clinical trials are being delayed at present and are playing clarification tennis with the FDA. So while the record order book is great, it's being skewed more to the right of screen more than is typically the case. As a result management have guided clinical trials in 1H FY23 to be at a similar level to the half just ended. Although they hope some of the FY24 contracted revenue may be brought forward into 2H FY24, hope is not strategy and they aren't providing a full year outlook. Healthcare's contribution for the full year is expected to be similar to FY22, which is not surprising given how much of it is derived from Eisai royalties at this time.
The good news is that FY24 and FY25 look absolutely bumper at the moment. Per the graph below (bottom left) the revenue backlog in FY24 is already almost that of FY23 and FY25 isn't too far behind.

The other thing that stood out on the call was the mix of Cogstate's share of Alzheimer's trial market between phase of trial. Cogstate has grown their overall share of this market to 17% but even better is the fact that their market share in phase 1&2 is much higher than phase 3. So if some of those early trials get good reads and roll into much larger phase 3 trials it bodes well for Cogstate.
The company is eagerly awaiting imminent reads from three phase 3 Alzheimer's trials and has highlighted that a positive outcome for any of these would have a positive impact on both the Trials business and the Healthcare business.

Like anyone I'd love to own a company that grew 30% year on year like clockwork through all cycles and conditions. But it's just not realistic - it's not how the world works. For me likely softness in FY23 (flatish versus FY22) doesn't reflect on the company or management's execution and I will continue to hold.
EBITDA** : $13,009,201 . 5,711, . 737 7, . 297,464 up 127.8% . Net profit up 43% , EPS up 41.9%
happy hunting today Following Mondays market rout.
Microsoft Word - FY22 Media Release_final.docx (markitdigital.com)

My thoughts following the release of the Cogstate quarterly update and investor call:
- Financial results were basically within guidance
- One exception was operating cash which was strong at US$9.2m, versus guidance of $5m+
- The one knock on the update was slowing sales in the quarter. For the first time since I’ve been watching them they didn’t fill the top of the sales funnel as quickly as revenue flowed out the bottom. Brad acknowledged that but said there was “no trend to talk to” and “expect to see a stronger Sep qtr”. Of the $8.8m sales in the qtr, approximately half should be recognised in FY23
- Alzheimers clinical trials are becoming an ever greater proportion of trial sales (84.2% in FY22 versus 65.3% in FY21)
- Seeing some delays in trials, which they attributed to delays in drug manufacture and recruitment of cohorts). They confirmed in Q&A that postponed trials delays not only revenue recognition but also cashflow as contract schedules are linked to milestones rather than dates.
- Noted near term readouts of phase III trials for Eisai and Roche (both CY22) and Lilly (mid 2023)
- Healthcare deal with Eisai will benefit from a successful phase III trial
- Noted that clinical trials are increasingly adding decentralised elements, which Cogstate are well positioned to support. Decentralised trials are cheaper overall but they believe Cogstate will get a larger proportion of the trial budget.
- When asked about margins they stated they were optimised for the current revenue base but should see further operating leverage on higher revenues. Also said a successful phase III trial would be beneficial for this as it would result in higher Healthcare revenue, which lends itself to more of a pure software sale rather than Clinical Trials, which are a mix of software and services.
- Proposed use of free cash flow – looking at acquisitions but they would need to be complementary to existing business and not add significantly to cost base. Otherwise there may be an opportunity to return some to shareholders.
- They didn’t mention the recent discussions throwing doubt on amyloid research published back in 2006 that Nnyck777 mentioned a few days ago (I did ask but they didn’t take that question).
Overall, I think it's a strong result showing that they are growing, are delivering operational leverage as they grow and some near term catalysts that would be very positive should they occur. The one thing that gives slight pause is the slowdown in contracted sales and I'll be watching the next quarterly closely to ensure it's a blip and not a trend.


[Held]
The trend on the CGS chart looks ok SMA50 could set-up for the SMA 200

Cogstate provided an update today, which re-iterated current year guidance but showed a significant increase in contracted revenue to be recognised in coming years.

It takes a little bit to get your head around this company, in particular the sizable moat that I argue it has and also how it's contracted revenue gets recognised over multiple years. However, once you do I think you find a really interesting company with some bright future prospects. I would say that it doesn't scream 'bargain' at me right now and it is quite volatile so you can afford to be picky with your entry.
The following slide is one I hadn't seen before and gives some more transparency about the lag between contracted revenue and revenue recognition:

If you are new to this one there's loads of posts about this on the company page. I'd also recommend the discussion Matt Joass had with the Overlord on the Meetings tab and also the Baby Giants podcast which covered it.
[Held]
Up to $2.47 so yes....
Snap shot of the Quaterly Result here for perusal,

There's been talk on Cogstate's valuation - how it's high and has a lot of the direct to consumer/doctor upside priced in.
I actually think the opposite is true - the valuation is very reasonable on the clinical trials business alone.
Right as of this moment, the company has more clincial trial contracted revenue in FY22 (USD$30.5m) and FY23 (USD$29.5m) than recorded in FY21. Through the last set of presentations, management is pretty much guiding $47-$55m group revenue (+48-74% growth) with no upside from the Healthcare segment. It's growing very quickly, and there's more visibile than ever.
I've included a "cohort" chart of contracted clinical trial revenues, and how it grows over the years. FY22 and FY23 numbers are of course my own forecasts. The assumptions in my opinion are quite balanced. All numbers are in USD.
On these numbers the company is currently trading at FY23 4.2x sales and 13x EV/EBIT. Again zero upside on the direct to consumer/doctor healthcare segment is built in.
